Reforming the Diagnostic Approach to Postpartum Psychosis
Postpartum psychosis (PP) is a rare yet severe psychiatric condition that demands immediate attention, yet its classification has long been mired in ambiguity. In recent discussions among experts, there has been a strong call to recognize PP as its own diagnostic category in the DSM. Proponents for this change argue that distinguishing PP from other mood disorders is essential to ensure that mothers receive the most effective treatment and support specific to their unique challenges after childbirth.
By drawing a clear line between PP and other mental health conditions, clinicians, researchers, and policy makers could steer through confusing bits of diagnosis and treatment plans more easily. This reclassification could also signal to the broader healthcare community that there are specific risk factors, treatment needs, and urgent care protocols associated with postpartum psychosis.
Understanding Postpartum Psychosis: Background and Urgency
The rapid onset and distinct clinical profile of postpartum psychosis require both immediate attention and specialized handling. Unlike other psychiatric conditions that might have a more gradual onset or a diffuse set of symptoms, PP typically occurs suddenly after childbirth, putting both the mother and child at significant risk.
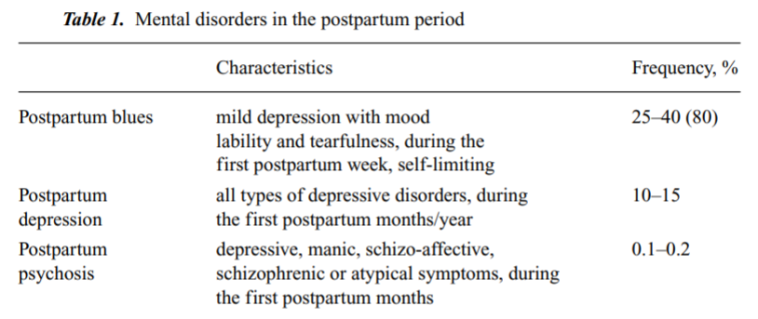
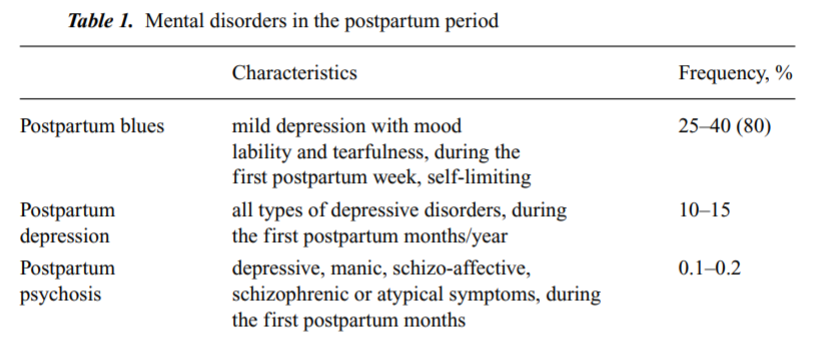
At first glance, women who have not previously experienced mental health issues may suddenly show symptoms that are both aggressive and alarming. The condition is estimated to affect about 0.1% to 0.2% of new mothers, yet its impact is disproportionate when considering its potential for tragic outcomes, including suicide and infanticide.
Distinct Onset and Symptom Presentation
One of the most compelling arguments for reclassifying PP is its unique onset after childbirth. Unlike mood disorders that may appear during pregnancy or extend from prior mental health issues, PP typically strikes immediately post-delivery. This timing is critical because it correlates with a period of significant hormonal, physical, and emotional changes in the mother.
Here are some of the subtle parts and fine shades that set postpartum psychosis apart:
- Sudden Onset: Symptoms often appear within the first few weeks postpartum, a period when new mothers are adjusting to major lifestyle changes and physical recovery from childbirth.
- Unique Symptom Profile: While mood disorders might share overlapping symptoms, PP frequently involves hallucinations, delusions, and extreme mood swings that require immediate redirection.
- Distinct Course: Unlike bipolar disorder or postpartum depression that may present a more gradual progression, PP is characterized by a rapid escalation that can leave little time for early intervention.
Diagnostic Challenges in Postpartum Mental Health
Recognizing and diagnosing postpartum psychosis comes with its own set of tricky parts and tangled issues. Many healthcare providers struggle to quickly identify PP, partly because the clinical presentation can overlap with normal postpartum adjustments. Additionally, since most mothers are at home during the onset of symptoms, early warning signs can easily be mistaken for common postpartum stress or fatigue.
The current DSM primarily features a peripartum specifier for mood disorders, which covers the period during pregnancy and the first four weeks after birth. However, this framework does not adequately capture the unique aspects of PP, which only occurs after childbirth. This gap in diagnosis is further complicated by assumptions that the disruptive emotional state is simply a part of the broader spectrum of postpartum experiences.
Tangled Issues in Recognizing the Signs
There are several confusing bits and twists and turns in the early identification of PP. Because the onset of symptoms occurs when new mothers are already under immense physical and emotional pressure, warning signs such as extreme mood swings, confusion, and delusional thinking are sometimes dismissed as transient or typical postpartum stress.
In practice, many women might not even report their experiences for fear of stigma or because they are overwhelmed by other changes in their lives. Several key challenges to timely diagnosis include:
- Home Environment Overlook: Symptoms often develop when women are recuperating at home, away from the structured environment of a hospital where signs are more likely to be recognized.
- Normalization of Stress: The significant psychosocial adjustments that accompany new motherhood can lead clinicians and family members alike to downplay early symptoms, attributing them to temporary stress rather than a serious condition.
- Overlap with Other Disorders: The subtle details of PP may mimic features of bipolar disorder or severe mood depression, making it essential yet challenging to isolate the diagnosis.
Symptom Overview Table
| Symptom | Description | Implication |
|---|---|---|
| Hallucinations | Sensory alterations including hearing or seeing things that are not present. | Indicates a dissociation from reality, requiring urgent intervention. |
| Delusions | Strongly held beliefs that are contrary to reality. | Signals severe disorientation that may affect the safety of both mother and child. |
| Mood Swings | Rapid and extreme changes in emotional states. | Reflects instability that complicates everyday functioning. |
| Confusion | Difficulty in understanding common situations. | May mask itself as typical postpartum fatigue, hence delaying diagnosis. |
Essential Treatment Strategies and Management Approaches
Due to its rapid onset and potential for serious harm, postpartum psychosis needs an urgent treatment strategy that differs from standard postpartum depression care. Experts recommend that once PP is suspected or diagnosed, the patient should immediately receive intensive and comprehensive care.
The treatment strategy anchored in current clinical research includes a stepwise approach involving inpatient care followed by a combination of medications. This approach is designed to manage the condition’s severity while reducing the likelihood of relapse in the critical postpartum period.
Immediate Intervention and Inpatient Care
Given that PP is classified as a psychiatric emergency, the initial response requires swift admission to a hospital setting where the condition can be closely monitored and addressed. New mothers experiencing PP should be moved into an environment that mitigates external stressors while allowing medical professionals to focus solely on stabilization and recovery.
Key components of immediate treatment include:
- Short-Term Benzodiazepines: Used to calm acute agitation and reduce immediate distress in a controlled setting.
- Antipsychotic Medications: Often administered to manage delusions and hallucinations, facilitating a clearer mental state.
- Lithium Therapy: Proven both to treat the current episode and to serve as a preventive measure against relapse within the first year postpartum.
Evidence from the largest study conducted on PP patients reported remission in 98% of cases with inpatient care following this structured treatment plan. This impressive rate of remission underscores the importance of a tailored approach.
Risk Factors and Prevention: A Closer Look
Preventing the onset or recurrence of postpartum psychosis involves identifying high-risk individuals and implementing proactive strategies to support women during the vulnerable phases of postpartum recovery. It is crucial to understand that certain risk factors elevate the chances of PP significantly.
Some of the key risk factors include:
- Prior Bipolar Disorder: Women with a history of bipolar disorder face about a 10-fold increased odds of developing PP during the postpartum period.
- Previous Postpartum Psychosis: A history of PP raises the risk further, making it even more critical to monitor these patients closely.
- Severe Mood Disorders: There is evidence suggesting that mothers with severe mood swings during pregnancy or postpartum are particularly vulnerable.
In addition to pharmacological interventions, a comprehensive care plan that encompasses nutritional support, counseling, and family education is essential. Women and their support systems must be made aware of the potential for rapid escalation and the need for immediate professional care.
Identifying High-Risk Groups: Factors to Consider
Discerning which women are more likely to experience PP is not straightforward due to the subtle differences and small distinctions in symptoms and history. However, careful assessment of risk factors can help healthcare providers to figure a path toward early intervention. The following considerations are critical when evaluating risk:
- Historical Mental Health Background: A previous diagnosis of bipolar disorder or mood dysregulation can serve as an important indicator.
- Family History: A documented history of severe mood disorders or psychiatric illnesses within the family can heighten risk levels.
- Symptom Monitoring Post-Delivery: Frequent check-ins during the first month postpartum can help in noticing rapid shifts in mental health status.
Early intervention, coupled with patient education, could be the key to reducing the incidence and severity of PP. A clear and empathetic communication strategy that explains the risks and necessary precautions is equally critical.
Comparative Outcomes and Remission Rates
The high success rate associated with structured treatment for postpartum psychosis highlights the critical need to treat it as a stand-alone disorder. Detailed studies suggest that with timely admission and a systematic, stepwise approach, nearly all patients can achieve remission.
In one of the largest studies on PP, a stepwise treatment model was linked to a 98% remission rate, underscoring the effectiveness of inpatient care and carefully managed medication protocols.
Clinical Remission and Stepwise Therapy
The approach to PP involves several distinct steps that can be summarized as follows:
- Immediate Evaluation: Rapid assessment upon hospitalization, including a full psychiatric evaluation and monitoring of vital signs.
- Pharmacological Stabilization: Initiation of short-term benzodiazepines to provide immediate relief from severe agitation.
- Targeted Antipsychotic Treatment: The administration of antipsychotics to control delusions and hallucinations while maintaining a safe environment.
- Lithium Addition: Introduction of lithium therapy to stabilize mood and reduce the risk of relapse, significantly enhancing the prognosis over the first postpartum year.
Below is a comparative table summarizing the treatment strategy and its reported outcomes:
| Treatment Step | Description | Outcome |
|---|---|---|
| Immediate Evaluation | Rapid hospitalization and psychiatric assessment | Quick stabilization and identification of PP |
| Benzodiazepines | Short-term use to calm acute symptoms | Reduced agitation and distress |
| Antipsychotic Use | Management of delusions and hallucinations | Enhanced clarity of thought and decrease in psychotic features |
| Lithium Therapy | Prevention and stabilization of mood swings | Reduced relapse rates and high remission within the first year |
Policy Implications and the Need for DSM Reclassification
The current classification schema does not sufficiently acknowledge postpartum psychosis as an independent disorder. Given the complexity of PP and its severe ramifications on maternal and infant health, there is a strong case to be made for a distinct diagnostic code in the DSM. Such a change would not only promote more detailed research but also standardize treatment protocols across the board.
As it stands, the peripartum specifier lumps together a wide range of mood disorders that vary greatly in onset and severity. Recognizing PP as a separate entity would allow clinicians to differentiate between a condition that may necessitate urgent inpatient care and other mood disorders with less immediate risks.
How Clear Classification Can Improve Patient Care
Designating postpartum psychosis as its own disorder can have several super important benefits:
- Streamlined Diagnosis: With clear criteria established for PP, healthcare providers can more quickly figure a path toward accurate diagnosis and optimal care.
- Tailored Treatment Plans: With an independent classification, treatment can be specifically designed to address the peculiar challenges of PP rather than applying generalized treatments used for broader mood disorders.
- Improved Prevention Strategies: Awareness of PP as a distinct disorder would encourage closer monitoring and preventive measures among high-risk groups, potentially saving lives.
- Enhanced Research Focus: A separate DSM category would likely spur more in-depth research into the causes, progression, and most effective therapies for PP.
Impacts on Maternal and Infant Safety
The stakes in postpartum psychosis are extremely high. The condition poses severe risks not only for the mother—through an increased chance of suicide—but also for the infant, with the potential for infanticide and other forms of harm. Additionally, children may end up displaced from their mothers, highlighting the far-reaching consequences of this disorder.
Maternal mortality related to PP is particularly alarming. Review committees in the United States have noted that many of these tragic outcomes are avoidable with prompt detection and treatment. The risk profile for PP clearly indicates that failure to address its specific challenges can result in preventable calamities.
Maternal Mortality and Preventable Risks
Recognizing PP as a separate disorder would enable clinicians to take more decisive action when warning signs emerge. Key issues include:
- Increased Risk of Suicide: PP is the leading cause of maternal mortality among preventable psychiatric conditions. Prompt intervention is crucial to mitigate this risk.
- Infanticide Prevention: Specific treatment protocols, when applied without delay, can forestall the harrowing outcomes of infanticide associated with untreated PP.
- Child Displacement: Unaddressed maternal mental health issues have significant repercussions for infant well-being, including the risk of the child being placed in out-of-home care.
A Holistic Approach to Postpartum Mental Health
The calls for reclassification of PP provide an important opportunity to reevaluate how we view and manage maternal mental health. In addition to targeted pharmacological interventions, a holistic care model is needed that integrates multiple aspects of health. This includes nutritional support, psychosocial counseling, and consistent postpartum monitoring.
Postpartum care should not be treated as a monolithic experience. Instead, it must be regarded as a mosaic of interlinked components, where physical recovery, mental health, and nutritional well-being all come together to form a complete picture of recovery and prevention.
Integrating Medical, Nutritional, and Psychosocial Support
For a truly effective approach to preventing and managing PP, the following strategies should be put into action:
- Robust Screening Programs: Establishing routine mental health assessments in the weeks following childbirth will ensure that any emerging symptoms are promptly addressed.
- Nutritional Counseling: Proper nutrition can play a role in stabilizing mood and energy levels. Diets rich in omega-3 fatty acids, vitamins, and balanced macronutrients provide essential building blocks for brain health during this challenging phase.
- Psychosocial Counseling: Immediate access to counseling services can help new mothers manage overwhelming feelings, reducing the likelihood that symptoms will escalate into full-blown psychosis.
- Family Education Programs: Educating family members and partners about the fine points of PP ensures that the home environment is supportive and that warning signs are recognized and acted upon quickly.
Conclusion: Taking the Wheel in Maternal Mental Health Care
In conclusion, the reclassification of postpartum psychosis as its own disorder is a step that could radically transform care for new mothers. By clarifying the diagnostic criteria, healthcare providers can more accurately figure a path toward early intervention and effective treatment, preventing the devastating consequences that PP poses for both mothers and their infants.
It is essential that stakeholders — from mental health professionals and obstetricians to policy makers — take a closer look at the evidence supporting distinct treatment pathways for PP. Not only is prompt and targeted intervention critical to reducing maternal mortality, but it also has the potential to improve the overall quality of life for countless families.
Ultimately, rethinking the diagnostic and treatment paradigms for postpartum psychosis represents more than just an academic exercise. It is about embracing a super important change that prioritizes the safety, well-being, and recovery of women during one of the most challenging periods of their lives. By taking a holistic and individualized approach to care, we can ensure that every mother receives the attention and treatment she deserves, preventing tragic outcomes and laying the groundwork for a healthier future for families worldwide.
As we continue to dig into the research and refine our therapeutic strategies, the healthcare community must steer through the tricky parts and tangled issues associated with postpartum mental health with empathy, precision, and urgency. Recognizing PP as a distinct disorder in the DSM is not just a bureaucratic change—it is a life-saving decision that could transform maternal mental health care for the better.
Originally Post From https://www.contemporaryobgyn.net/view/experts-recommend-postpartum-psychosis-be-classified-as-its-own-disorder
Read more about this topic at
Postpartum Psychosis: International Experts Seek to Save …
Experts recommend postpartum psychosis be classified as …
