Central Retinal Artery Occlusion: An Urgent Call for Action
Central retinal artery occlusion (CRAO) is a clear, albeit nerve-racking, reminder of how swiftly our health can be affected by vascular issues. As an ophthalmic emergency that leads to sudden, painless loss of vision in one eye, CRAO demands that both the public and healthcare professionals stay alert. I want to take a closer look at the current practices, emerging therapies, and the tricky parts related to emergency management of CRAO, so that we can all better understand this condition’s far-reaching implications.
In our busy emergency departments (EDs) and clinics, CRAO is often caught in a chaotic race against time – a race where every minute counts. Despite our advanced medical technologies and increasing public awareness about stroke, the tangled issues associated with CRAO management continue to challenge us. In this editorial, I’ll dive into the fine points of what we know about CRAO, outline the state-of-the-art diagnostic methods, and discuss promising emerging therapies that could steer our way toward better outcomes.
Understanding the Foundations of CRAO
CRAO happens when an obstruction in the central retinal artery stops blood from reaching the retina – the light-sensitive tissue at the back of the eye. Without this crucial blood supply, the retina rapidly suffers from ischemia, leading to irreversible damage. The condition is often related to embolic events, inflammatory processes, or hypercoagulable states, meaning that the underlying causes are diverse and complex.
Some of you might wonder what exactly complicates CRAO management. The answer lies in the delicate anatomy of the eye. For example, while the inner two-thirds of the retina depend exclusively on the central retinal artery, the outer portion – including the light-detecting photoreceptors – receives blood from the choroidal circulation. This unique dual blood supply is one of the key reasons why CRAO can be both tricky and intimidating; the absence of collateral circulation in the inner retina means that even a small embolus can cause extensive damage.
Detailed Anatomy and Blood Supply Issues
Let’s break down how the retina receives blood:
- Central Retinal Artery: Supplies the inner layers of the retina, including the ganglion cell layer and nerve fiber layer.
- Choroidal Circulation: Delivers blood to the outer retina, particularly the photoreceptor layer.
- Cilioretinal Artery: In some individuals, this additional artery can offer a super important backup supply to the central retinal area, sometimes sparing the macula even when the central retinal artery is occluded.
This unique setup, while fascinating in its design, is also full of problems when things go wrong. Once the central retinal artery is blocked, the retina’s ability to function gracefully diminishes almost immediately, making prompt detection and intervention absolutely critical.
Emergency Diagnosis: Getting Into the Nitty-Gritty
Working through the pathway to a correct diagnosis of CRAO in the emergency room is often a challenge filled with twists and turns. Many patients with CRAO present with sudden, painless vision loss – a symptom some might easily dismiss as a temporary blackout. However, the stakes here are high, as even a short delay in treatment can lead to permanent blindness.
Recognizing the Early Signs and Symptoms
One of the subtle parts that many people miss is that vision loss in CRAO is abrupt and often accompanied by an afferent pupillary defect. In plain language, this means when light is shone in the affected eye, the pupil does not respond appropriately. Here are the key red flags:
- Sudden, painless vision loss in one eye
- Dark shadows or partial loss if a cilioretinal artery is present
- Delay in presentation to the emergency department – sometimes because the vision loss is not recognized as a true medical emergency
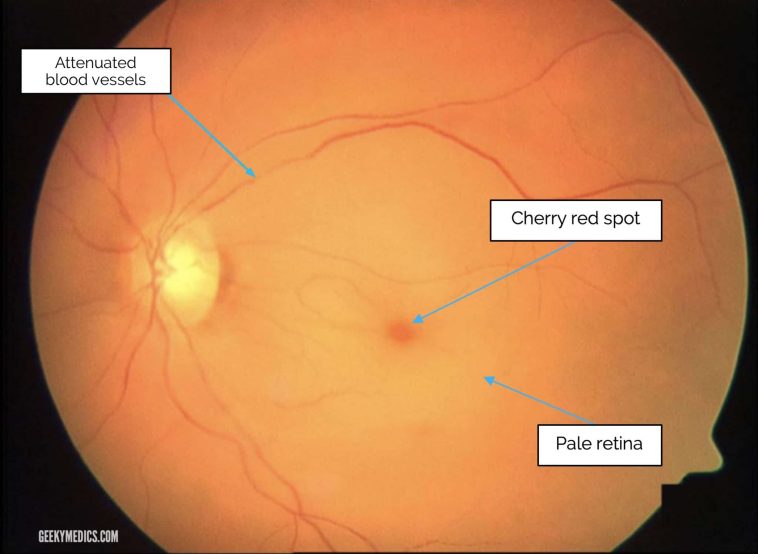
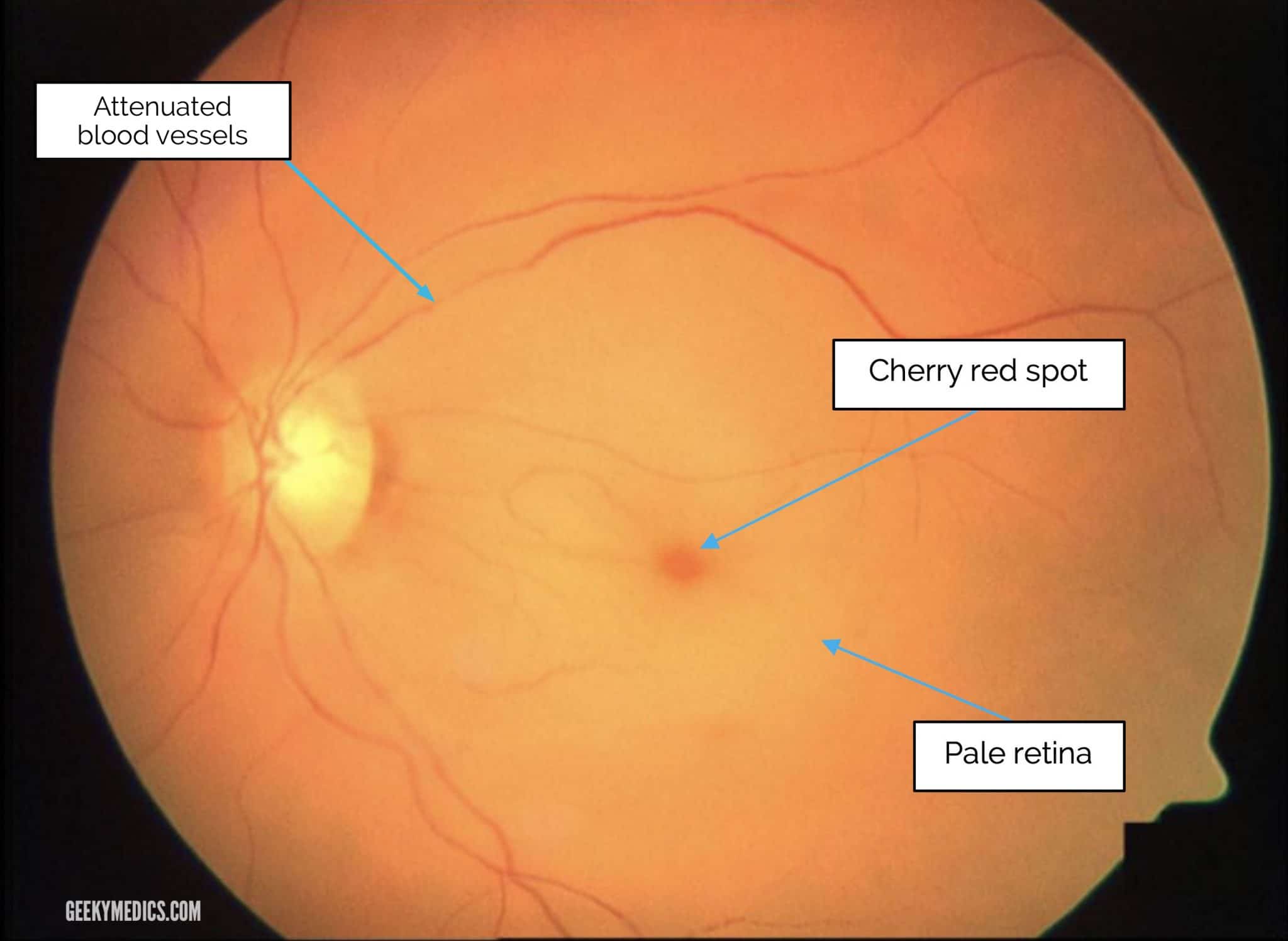
Emergency clinicians are urged to figure a path quickly by performing a thorough ocular exam including fundoscopic examination. Early retinal findings, such as the classic “cherry-red spot” on the macula, help confirm the diagnosis. However, in the first few hours after the occlusion, these signs might be less obvious.
Enhanced Imaging Modalities in the ED
Modern optical imaging techniques have greatly improved our ability to identify CRAO in what can sometimes feel like a nerve-wracking race against time. Some key diagnostic tools include:
- Optical Coherence Tomography (OCT): This imaging modality helps to detect inner retinal thickening and other subtle changes that occur during the acute phase of CRAO. OCT has become a super important tool, enhancing early detection and allowing specialists to make treatment decisions sooner.
- Fluorescein Angiography: This test reveals how blood flows through the retinal vessels and identifies areas of delayed filling. It’s critical for mapping out the extent of ischemia.
- Point-of-Care Ultrasound (POCUS): A handy, on-the-spot method that can sometimes pinpoint embolic material in the retrobulbar region, offering a quick, bedside diagnostic window.
Each of these modalities has its own set of challenges and benefits. For instance, while POCUS is readily available in many EDs, it requires a skilled operator and may not capture the fine details that OCT provides. In a hectic emergency setting, ensuring the availability and proper use of these technologies remains an ongoing process full of problems for many institutions.
Therapeutic Strategies: Sorting Out the Options
The available treatment options for CRAO continue to be a topic both of hope and frustration. Despite various interventions proposed and tried over the years, many lack robust evidence from large-scale randomized controlled trials. As such, physicians are often left working through a process of trial and error – a nerve-racking situation in a condition where time is vision.
Conventional Interventions
Traditional approaches remain in use even though their effectiveness varies greatly. These methods include:
- Ocular Massage: The idea here is to use intermittent pressure on the eyelid, hoping to dislodge the embolus. While it’s a quick and accessible technique, its success is unpredictable and generally modest.
- Lowering Intraocular Pressure (IOP): Therapies such as carbonic anhydrase inhibitors (e.g., acetazolamide) and topical beta-blockers are used to reduce IOP and thereby possibly enhance retinal blood flow.
- Anterior Chamber Paracentesis: A procedure meant to quickly lower intraocular pressure by removing a small volume of aqueous humor, though it does carry minor risks.
- Hyperbaric Oxygen Therapy (HBOT): This involves breathing 100% oxygen under high pressure, with the goal of enhancing oxygen diffusion to the retina. Evidence from case series suggests an improvement in visual prognosis if HBOT is provided early enough.
Although these interventions are widely adopted, their overall impact on visual recovery has been mixed. Their limited success only further underscores the need to explore more promising, innovative treatments.
Emerging Treatments and Forward-Looking Approaches
Among the promising new approaches in the literature, targeted thrombolysis – using tissue plasminogen activator (tPA) either intravenously or even intra-arterially – has attracted significant attention. Some observational studies indicate that tPA might lead to improved visual outcomes when administered within a narrow time window. However, there is understandable hesitation due to the potential for serious hemorrhagic complications.
Other experimental strategies, such as:
- Nd:YAG Laser Embolysis: A technique using laser energy to break up emboli, which has shown success in individual cases where traditional methods have failed.
- Pars Plana Vitrectomy (PPV): In select cases, PPV combined with techniques for reducing IOP has shown promise in facilitating the breakdown of the embolus and restoring blood flow.
- Mesenchymal Stem Cell-Based Therapies: Early experimental models are exploring whether these cells, when administered into the vitreous humor, could reduce neuroinflammation and support retinal recovery following ischemic injury.
While these therapies are still in development and their long-term effects remain to be fully evaluated, they represent a hopeful frontier for a condition that has long been seen as one of the more intimidating challenges in ophthalmology.
The Role of Systemic Health and Preventive Strategies
One of the key factors that often remains overlooked is the critical connection between CRAO and systemic health conditions. CRAO is not just an isolated ocular problem; it is often a harbinger of wider cardiovascular issues.
Cardiovascular Risk Factors and Their Influence
Numerous studies show that CRAO has strong associations with systemic conditions such as:
- Hypertension
- Diabetes Mellitus
- Hyperlipidemia
- Atherosclerosis
Atherosclerosis, in particular, is a major contributor. Plaque buildup in the carotid arteries or even in the aortic arch can send embolic fragments to the eye, leading to occlusion. Given these connections, it is crucial that patients with CRAO are thoroughly evaluated for underlying systemic diseases.
Systemic Therapies and Long-Term Management
Considering the systemic nature of the factors at play, the use of antiplatelet agents like aspirin (and others such as clopidogrel) is a common practice to help protect the retina and reduce the risk of recurrent strokes. Additionally, anticoagulation therapy might be considered in cases with a cardioembolic source, such as atrial fibrillation.
The following table outlines common systemic interventions and their intended effects:
| Treatment | Purpose | Considerations |
|---|---|---|
| Aspirin/Clopidogrel | Reduce platelet aggregation and prevent further embolic events | Lacks conclusive trial data specifically for CRAO outcomes |
| Anticoagulation (Heparin/Warfarin) | Target cardioembolic risk, especially in atrial fibrillation | Risk of bleeding complications |
| Lifestyle Modification | Address hypertension, hyperlipidemia, and diabetes+ | Requires long-term patient commitment |
Preventive strategies are super important. Public health campaigns, continuous education for healthcare providers, and early screening in high-risk populations can all help reduce the risk of CRAO. In essence, the eye can sometimes serve as a “sentinel” for overall vascular health, and recognizing that connection allows for more timely, comprehensive intervention.
Delays in Care: Overcoming the Time Hurdle
One of the most challenging aspects of CRAO is the delay in seeking treatment. Many patients do not realize that sudden monocular vision loss is an emergency, often attributing it to less serious causes. This delay transforms an already tense situation into one loaded with issues, as the retina begins to suffer irreversible damage shortly after blood flow is obstructed.
Barriers to Timely Presentation
There are several reasons why patients may not present immediately to an ED:
- Lack of public awareness: Many people do not know that sudden vision loss in one eye is a medical emergency akin to a stroke.
- Geographical barriers: Rural areas and regions without specialized stroke or eye clinics may delay definitive diagnosis and management.
- Fear and confusion: When symptoms occur suddenly, the unexpected nature of the event itself can be off-putting, causing hesitation to immediately seek help.
Improved public education is key. Campaigns that stress “time is vision” must be implemented to encourage those experiencing sudden visual changes to immediately seek medical attention. As emergency departments evolve, establishing fast-track “Eye Stroke” protocols will be super important in reducing these delays.
Overcoming Infrastructural and Diagnostic Hurdles
The availability of advanced imaging in crisis situations is another tangled issue. Not every ED or clinic today has immediate access to OCT or non-mydriatic fundus photography. This lack of universal access can leave clinicians feeling on edge as they try to figure a path through a maze of diagnostic uncertainties.
To improve the situation, some potential solutions include:
- Telemedicine and Remote Consultation: By allowing retinal images to be reviewed off-site by specialists, images can be rapidly interpreted, thus reducing overall delays.
- Integration of Artificial Intelligence: Advanced algorithms trained on large datasets of OCT images could help flag potential cases of CRAO early, even before all the clinical signs fully develop.
- Standardized Protocols: Clear, streamlined protocols for managing suspected CRAO cases, similar to those for cerebral strokes, can help emergency teams work more efficiently.
These improvements are not just improvements in workflow; they are super important for potentially saving vision. With public and institutional commitment, we can better handle these nerve-racking diagnosis challenges and get patients into proper care faster.
Multidisciplinary Collaboration: A Must-Have Approach
One of the small distinctions that truly improves patient care in CRAO is the involvement of a multidisciplinary team. CRAO, with its web of ocular and systemic implications, demands that emergency physicians, ophthalmologists, neurologists, and internists work hand-in-hand to figure a path toward better outcomes.
The Importance of Coordinated Expertise
When a patient presents with a suspected CRAO:
- Ophthalmologists are needed to make a precise diagnosis using specialized tools and examinations.
- Neurologists contribute by evaluating the risk for concurrent cerebrovascular events and coordinating acute stroke protocols.
- Internists and Cardiologists focus on the systemic conditions that may have contributed to CRAO, such as uncontrolled hypertension or atrial fibrillation.
This coordinated care model, though it might seem like a complicated piece to manage in a busy hospital, is essential. Not only does it help save the patient’s eye, but it also acts as a wake-up call to address broader cardiovascular health issues.
Case Studies and Real-World Experiences
There have been several real-world cases where rapid, multidisciplinary intervention has made a dramatic impact. For instance, reports indicate that using advanced imaging techniques in stroke centers resulted in earlier detection of CRAO in up to 42% of cases – a statistic that is both encouraging and a reminder of the nerve-racking pace at which these events unfold.
In a particularly striking case, a patient with CRAO was treated promptly with a combination of ocular massage, IOP-lowering medications, and eventual thrombolytic therapy, resulting in a notable improvement in vision. Such cases highlight not only the potential of available therapies but also the need for improved coordination among various specialties.
Looking Ahead: The Promise of Future Innovations
The future of CRAO management is promising. With the rapid development of new technologies and the advent of innovative therapeutic approaches, we are beginning to see clear signs of progress. The following subtopics highlight some of the exciting directions in which we are headed.
Artificial Intelligence in Eye Imaging
AI-assisted diagnostics represent one of the most cutting-edge areas of research in the management of CRAO. Machine learning algorithms, when trained on thousands of OCT images, have the potential to identify subtle details that even experienced clinicians might miss. This technology could become a super important adjunct tool in the ED, reducing the time required for diagnosis and potentially opening up new treatment windows.
This is not just a futuristic dream – early studies indicate that AI can successfully distinguish between normal retinal anatomy and that affected by CRAO, providing a fresh pathway for rapid diagnostics in busy emergency settings.
Standardized “Eye Stroke” Protocols
Given the time-sensitive nature of CRAO, developing standardized protocols akin to those used in stroke management is essential. These protocols would involve:
- Rapid triage and evaluation of patients reporting sudden vision loss
- Immediate access to advanced imaging modalities
- Quick and coordinated multidisciplinary intervention
- Streamlined decision-making processes on whether thrombolytic therapies or alternative interventions should be pursued
Implementation of such “Eye Stroke” protocols could transform emergency care, ensuring that every minute is maximized in the fight to save vision.
Emerging Pharmacological and Surgical Interventions
In experimental settings, several new therapies are being explored. For example, intra-arterial thrombolysis using carefully dosed tPA holds promise if administered very early – though its widespread adoption will require more robust clinical data and carefully defined patient selection criteria.
Other promising interventions include:
- Laser Embolysis: Using laser energy to break up the embolus might remove an occlusion without the systemic risks associated with thrombolytic drugs.
- Pars Plana Vitrectomy Combined with Endovascular Approaches: This combined therapy seeks to relieve pressure and mechanically address the occlusion, representing an innovative approach that could offer another option for those who do not respond to conventional treatments.
The hope is that, as these emerging strategies are refined and validated through large clinical trials, they will soon offer us more reliable ways to salvage vision in patients with CRAO.
Conclusion: A Roadmap for Change and Hope
Central retinal artery occlusion remains one of the most challenging ophthalmic emergencies. Its management is loaded with issues – from recognizing the subtle beginnings of vision loss to overcoming diagnostic delays and choosing among various treatment options that have mixed results.
Yet, there is hope. Advanced imaging techniques, smart eye-stroke protocols, and emerging therapies like AI diagnostics and targeted laser treatments promise to reshape the way we address CRAO. However, the road ahead requires commitment – from both healthcare providers and policymakers – to educate the public about the urgency of vision loss and to invest in diagnostic and treatment technologies that can make a real difference.
As we witness ongoing research and clinical trials, it is clear that a multidisciplinary approach is a must-have in tackling CRAO. Only by working together can we figure a path through the twists and turns of this condition, ensuring that patients receive timely, effective care that not only saves vision but also enhances overall vascular health.
In the end, addressing CRAO requires us to embrace both the old and the new – to acknowledge the value of traditional interventions while being unafraid to try innovative therapies backed by modern technology. By doing so, we can transform a condition once seen as inevitably overwhelming into one where early detection and swift, coordinated care pave the way for meaningful recovery.
The collective goal should be clear: to reduce delays in care, improve diagnostic precision, and ultimately give patients a fighting chance at preserving their sight. With continued advances and increased awareness, CRAO management may one day shift from a nerve-racking emergency to a manageable medical situation, offering renewed hope for those at risk.
Key Takeaways in Managing CRAO
- Understanding the fine points of retinal blood supply is critical to grasping the severity of CRAO.
- Timely diagnosis in the ED – facilitated by advanced imaging techniques and AI assistance – can be a game changer.
- Multiple treatment strategies exist, yet a consensus on the most effective approach remains elusive.
- Systemic conditions such as hypertension, diabetes, and atherosclerosis play a major role in the development of CRAO and must be managed concurrently.
- Public education and standardized “Eye Stroke” protocols are incredibly super important to reducing treatment delays.
- Multidisciplinary collaboration is key; pooling the expertise of various specialists can yield the best outcomes.
In our increasingly interconnected and technologically advanced medical landscape, the future of CRAO care appears brighter than ever. But making that future a reality will require us all to recognize the early signs, act quickly, and invest in both research and collaborative care models. By taking these necessary steps, we can ensure that what was once a nerve-racking and overwhelming ordeal transforms into a condition where prompt action saves not only sight but lives as well.
Ultimately, addressing CRAO does more than save vision; it acts as a wake-up call for evaluating overall cardiovascular health. So, the next time you hear about sudden vision loss, remember – time is vision, and every moment counts. Let us pledge to stay informed, work together, and support the innovations that will pave the way for more effective treatments in years to come.
Originally Post From https://www.cureus.com/articles/407819-central-retinal-artery-occlusion-in-acute-care-current-practices-and-emerging-therapies
Read more about this topic at
Ocular Emergencies
Eye Emergencies: What to Do When Time Is of the Essence
